Carpal Tunnel Syndrome
- News
-
Jun 03
- Share post
Dear Sir
I am writing you about the Carpal Tunnel article appearing in the Spring 1997 issue of the Journal of the American Academy of Osteopathy. This exceptional article, appearing in the student’s corner and well-written by Kelly Miller, shows great thought and appreciation for the relevant anatomy involving osteopathic Carpal Tunnel Syndrome treatment. Ms Kelly rightly notes that releasing tension of the flexor retinaculum enlarges the carpal tunnel and helps remove pressure (compression neuropathy) of the Median Nerve. The home exercises reviewed here and others devleoped by Ben Sucher, D.O. offer great relief to Carpal Tunnel Syndrome sufferers.
I wish to add one other anatomical aspect of CTS etiology and describe a brief treatment that has helped my CTS patients. Of course, this aspect follows upon proper medical diagnostic evaluation and osteopathic treatment of the patient’s general and specific musculoskeletal strains and appropriate areas of somatic dysfunction.
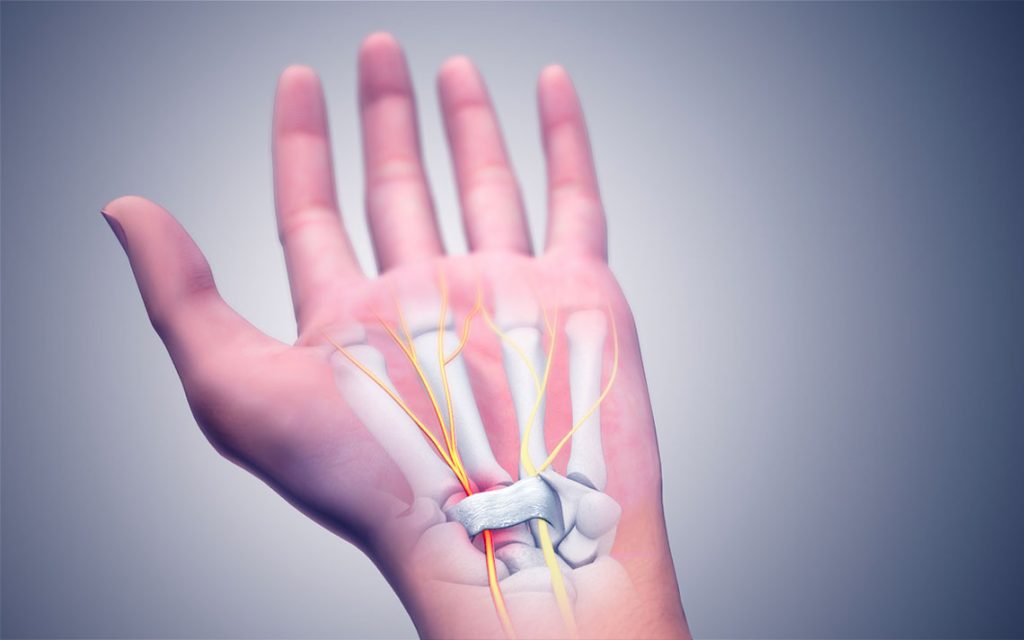
The treatment then focuses around the capitate as “troublemaker.” When the entire capitate bone translates toward the palmer surface or when the capitate body, rotating about the captate’s short transverse axis, moves toward the palmer surface, carpal tunnel stress ensues. The capitate’s malposition within the carpal tunnel makes it a “space occupying lesion.” The malpositioned capitate compresses the deep flexor tendons (flexor digitorum profundus) against the superficial flexor tendons (flexor digitorum superficialis). The whole tendon mass then pushes against the median nerve, superficial to them. The median nerve, the softest and most vulvnerable of the the prior structures, now becomes compressed against a relatively unyielding flexor retinaculum. Thus, entrapped and compressed, the median nerve complains, producing those familiar Carpal Tunnel Syndrome symptoms of which our patients complain.
Following this anatomical reasoning so far, it is now time to do something about our “carpal tunnel troublemaker” – diagnosis and treatment. A malpositioned capitate may be easily diagnosed as an unusual depression on the dorsum of the hand at the base of the third metacarpal. You can detect this unusual depression by comparing normal and CTS symptomatic patients. After a while, the differences between normal and abnormal depth, tissue elasticity, texture changes and resiliency, not to mention motion, (somatic dysfunction) become immediately apparent.
Treatment consists of simply analyzing the bony malalignment and correcting it with whatever manipulative paradigm works best for you. A technique that I have found helpful follows:
1. Place an index finger on the dorsum of the wrist on the distal end of capitate body and the thumb of the same hand on the capitate body, palmer surface. That is, the distal end of capitate body is held between the thumb and index finger.
2. With the free hand, hold the distal phalanges of the second, third and fourth digits. Apply traction, localizing your tension to the capitate carpal joints just distal to your capitate handhold.
3. With a direct or indirect action maneuver, reposition (translate, de-rotate, de-twist) the capitate to its proper or more proper anatomical relationship.
4. Now that the capitate is in its more normal anatomical relationship, check to see if the “depression” at the base of the third metacarpal has “filled in.”
5. Finally, normalize, if necessary, the relationship between capitate head and lunate.
I hope these few osteopathic thoughts add a few more percentage points to our reader’s Carpal Tunnel Syndrome successes. I thank Ms Kelly for her well-written and well-researched article.
Stephen M. Davidson, D.O., CSP-OMM